Why choose Mr Henderson for paediatric retinal disease?
Mr Henderson founded the vitreoretinal unit at Great Ormond Street Hospital and is one of fewer than five surgeons in the UK performing vitreoretinal surgery on infants. GOSH is the UK’s national referral centre for paediatric retinal disease, receiving referrals from across the United Kingdom and internationally. Refer your patient or enquire directly.
Paediatric Vitreoretinal Surgery
Children with vitreoretinal conditions require specialist expertise that bridges adult retinal surgery and paediatric medicine. As Consultant Vitreoretinal Surgeon and Clinical Lead for Ophthalmology at Great Ormond Street Hospital, Mr Henderson provides this uniquely specialised care.
Paediatric Retinal Surgery at GOSH
Great Ormond Street Hospital is one of the world’s leading centres for children’s medicine and surgery. Mr Henderson leads the ophthalmology service, managing the full range of paediatric vitreoretinal conditions that require the combined skills of an experienced retinal surgeon with an understanding of the unique challenges of operating on a child’s eye.
Children are not simply small adults — their eyes are still developing, their cooperation during examination is limited, and many conditions seen in paediatric practice are not encountered in adults. The surgical techniques, anaesthetic approach, and postoperative management must all be adapted accordingly.
“Operating on a child’s eye is amongst the most demanding work in vitreoretinal surgery. The stakes are enormous — restoring or preserving vision in a child can change the entire trajectory of their life.”

Paediatric Conditions
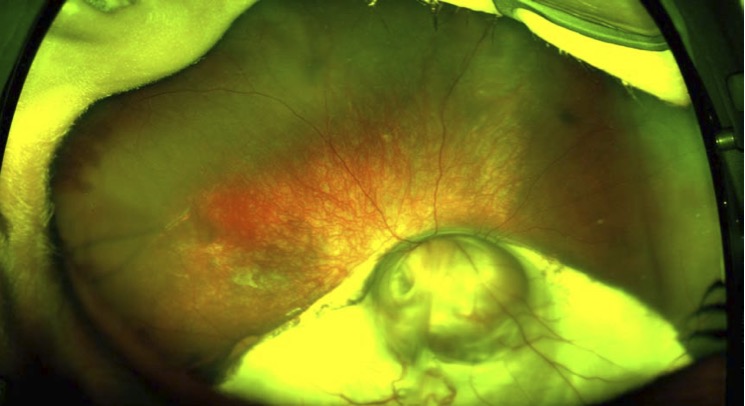
Coats Disease
An idiopathic retinal vascular condition causing exudation and exudative retinal detachment. Treated with laser, cryotherapy, and intravitreal injections. Surgery for advanced cases.
Coloboma
A congenital gap in the retina, choroid, or optic nerve caused by incomplete fusion of the optic fissure. Surveillance for retinal detachment and management of associated complications.
Paediatric Retinal Detachment
Rare but sight-threatening. Often associated with genetic conditions, trauma, or extreme prematurity. Requires technically demanding vitrectomy surgery.
Inherited Retinal Dystrophies
Early-onset conditions including LCA, CRB1 dystrophy, and Stargardt disease. Diagnosis, surveillance, genetic counselling, and access to gene therapy where eligible.
Familial Exudative Vitreoretinopathy
A genetic condition affecting retinal vascular development, causing a spectrum from mild peripheral avascularity to severe tractional retinal detachment.
Retinopathy of Prematurity
A potentially blinding condition affecting premature infants. Management in collaboration with the neonatal team, including laser treatment and surgery for advanced cases.
“Our daughter was diagnosed with a retinal condition at eight years old. Mr Henderson at GOSH was extraordinary — calm, thorough, and genuinely caring. He explained everything in a way we could understand, and our daughter trusted him completely. We felt we were in the very best hands.”
Arrange a Consultation
Mr Henderson personally sees and treats all paediatric patients at GOSH. As Clinical Lead for Ophthalmology, he brings the full resources of the hospital to every child’s care.
To arrange an assessment for a child with a vitreoretinal condition, please contact Alison Anscombe, Mr Henderson’s secretary:
+44 7974 015691 · alison.anscombe1@nhs.net
Or use the contact form on this website. Referrals from GPs and other specialists are welcome.