Why choose Mr Henderson for macular hole surgery?
Mr Henderson has an extensive personal series of macular hole repairs with closure rates consistently above 90%. He performs minimally invasive 25-gauge vitrectomy with ILM peel and avoids prolonged face-down positioning wherever possible. All surgery is performed personally at Moorfields Eye Hospital by a dedicated consultant retinal surgeon in London.
Macular Hole Surgery in London
A macular hole is a small but significant defect at the very centre of the retina that causes a characteristic loss of central vision. Surgery to close the hole is highly successful, with closure rates exceeding 90% in most cases.
What is a Macular Hole?
The macula is the central part of the retina responsible for detailed, straight-ahead vision — reading, recognising faces, and watching television. At its very centre lies the fovea, where visual acuity is sharpest.
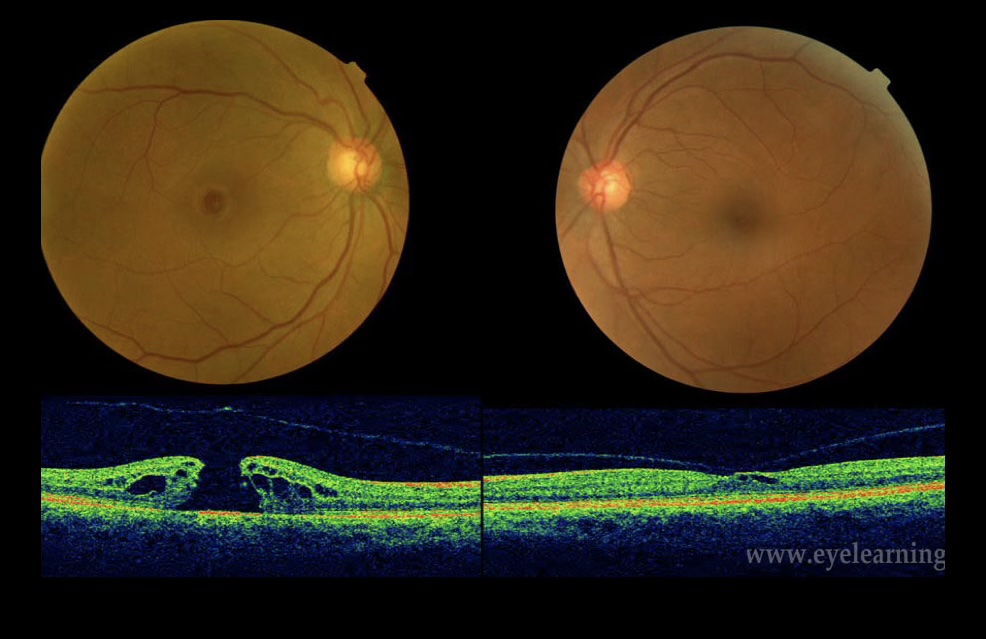
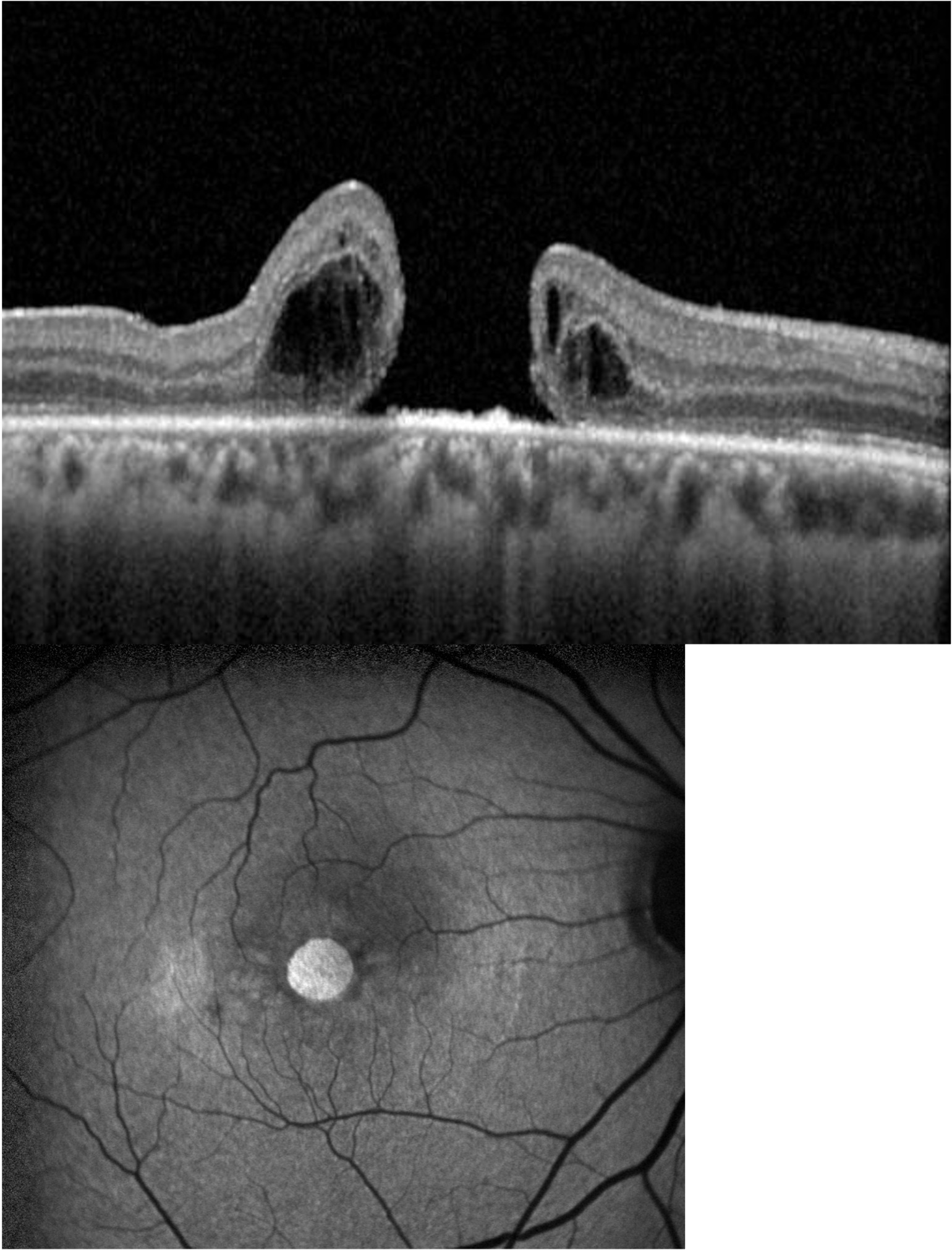
A macular hole is a full-thickness defect through all layers of the retina at the fovea. It forms when the vitreous gel pulls away from the retinal surface abnormally, exerting traction on the delicate foveal tissue until it tears through.
Macular holes most commonly occur in people over 60 and are more common in women. In most cases there is no underlying cause — they arise spontaneously as part of normal vitreous ageing.
Symptoms of a Macular Hole
Symptoms develop gradually over weeks to months. Because only the very centre of vision is affected, peripheral vision remains intact — but the impact on daily life can be profound.
Surgery for Macular Hole
Vitrectomy surgery achieves closure in over 90% of cases. Mr Henderson performs minimally invasive 25-gauge vitrectomy, removing the vitreous gel and carefully peeling the internal limiting membrane (ILM) from the retinal surface. This relieves traction on the hole and allows it to close.
“The choice of posturing, gas, and whether amniotic membrane is needed is determined by the precise size of the hole — not a one-size-fits-all protocol.”
The eye is filled with a gas bubble to provide gentle support while the hole heals over the following weeks.
Posturing & Advanced Techniques
Your Journey from Diagnosis to Recovery
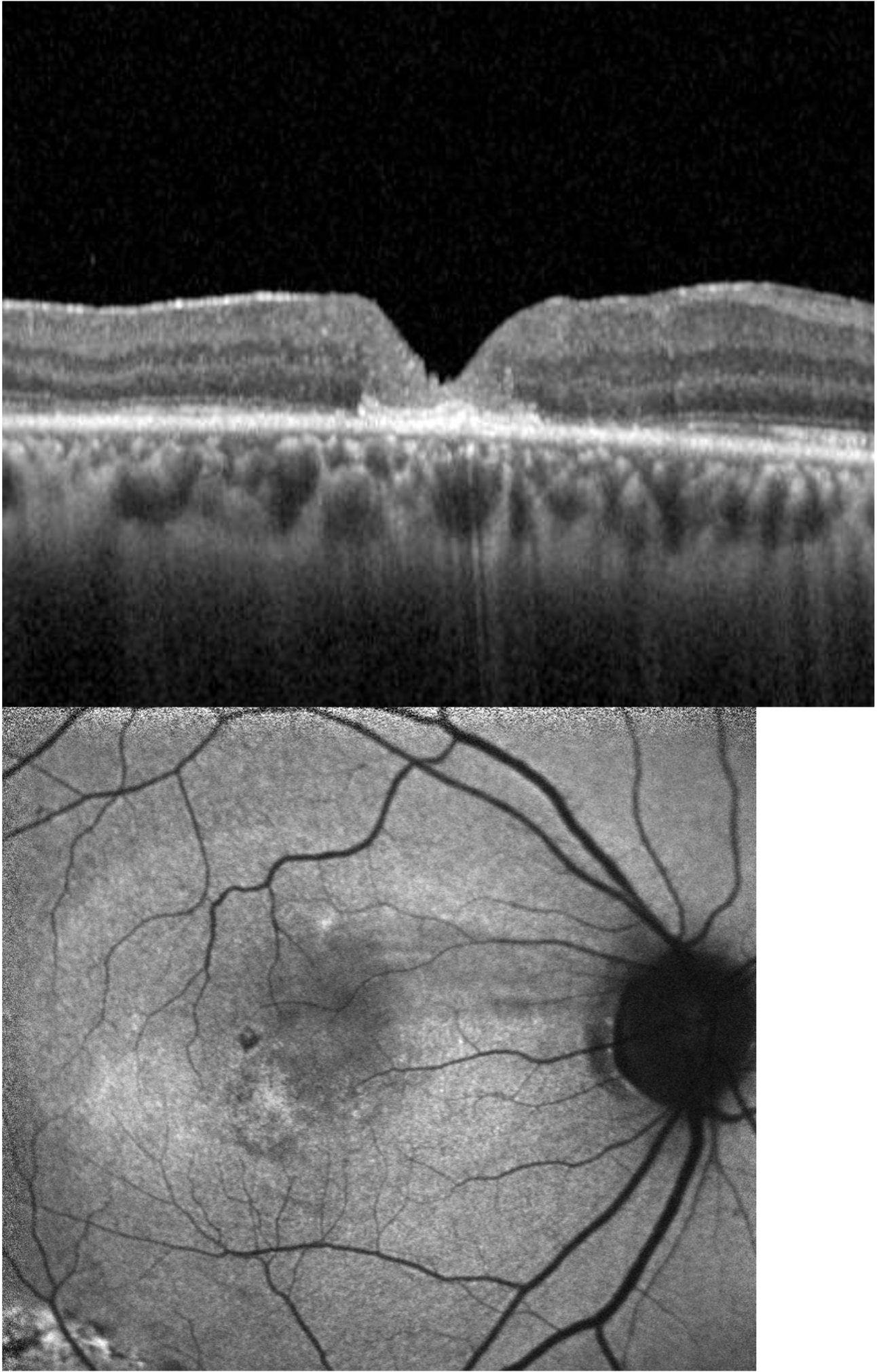
OCT imaging precisely measures the hole — size determines the surgical plan. A clear diagnosis and honest assessment at the first visit.
Mr Henderson tailors posturing, gas type, and technique to your specific hole size — including amniotic membrane for large or recalcitrant holes.
Minimally invasive 25-gauge vitrectomy at Moorfields, performed personally by Mr Henderson. Most patients go home the same day.
Vision improves gradually over weeks to months. Mr Henderson monitors your recovery personally with structured follow-up appointments.
Small & Medium Holes
Strict face-down posturing is not required. Remaining still and looking slightly downward allows the gas bubble to maintain contact with the hole.
Large Holes (>600 μm)
Evidence supports face-down posturing for a defined period. Mr Henderson provides clear written instructions tailored to your specific hole size.
Very Large / Recalcitrant (>1000 μm)
Subretinal amniotic membrane transplantation is offered, achieving closure in almost all cases with a meaningful improvement of approximately two lines of vision.
Frequently Asked Questions
“I had been told I might never read properly again. After Mr Henderson operated on my macular hole at Moorfields, my reading vision has recovered to the point where I no longer need a magnifier. The care and explanation throughout were exceptional.”
Arrange a Consultation
Mr Henderson personally performs all macular hole surgery. There is no delegation to junior colleagues.
To arrange an assessment for macular hole, please contact Alison Anscombe, Mr Henderson’s secretary:
+44 7974 015691 · alison.anscombe1@nhs.net
Or use the contact form on this website.