Why choose Mr Henderson for vitreous floaters?
Mr Henderson is one of a small number of UK surgeons who offers vitrectomy for significant symptomatic floaters. He takes a careful, conservative approach — surgery is only recommended when floaters are genuinely disabling — but when it is indicated, outcomes are excellent. All surgery is performed at Moorfields Eye Hospital. Discuss your symptoms with a specialist retinal surgeon in London.
Vitreous Floaters
Most floaters are benign and represent normal age-related changes to the vitreous gel. However, a sudden onset of new floaters — particularly if accompanied by flashing lights — requires urgent assessment to exclude a retinal tear or detachment.
Understanding Vitreous Floaters
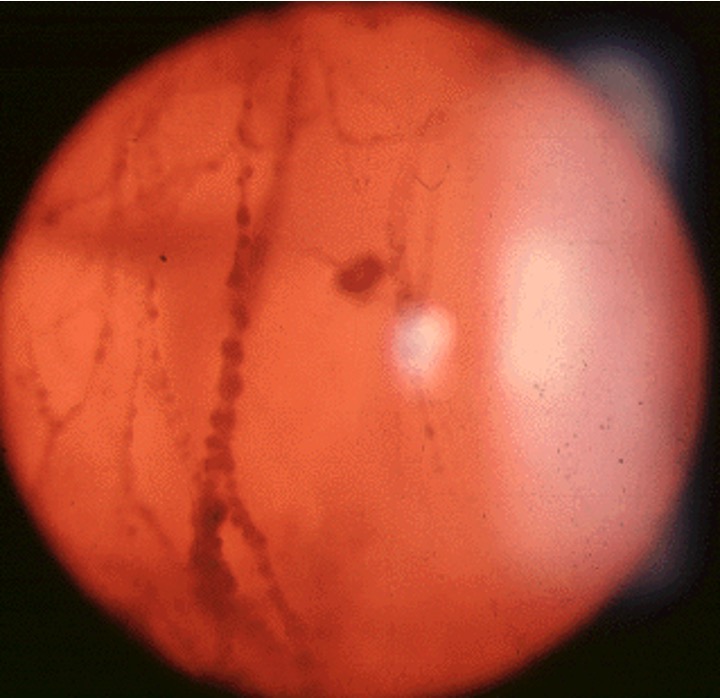
Floaters are shadows cast on the retina by condensations or opacities within the vitreous gel — the clear jelly that fills the eye. They appear as spots, threads, cobwebs, or rings that drift across the visual field, particularly noticeable against bright backgrounds such as a clear sky or white page.
The most common cause is a posterior vitreous detachment (PVD) — a normal age-related process in which the vitreous gel separates from the retinal surface, usually occurring in people over 50. The separation creates a ring-shaped condensation (Weiss ring) that can cause a prominent floater.
Most floaters caused by PVD are harmless. The brain gradually learns to ignore them, and for most patients they become less noticeable over several months.

Severe or Symptomatic Floaters
A minority of patients have floaters that are sufficiently large, dense, or persistent that they cause significant and ongoing visual impairment. In these cases, vitrectomy surgery can be considered.
Vitrectomy removes the vitreous gel and its contents — including the floaters — and replaces it with a clear saline solution. In experienced hands it is highly effective at eliminating floaters. The risks of surgery must be carefully weighed against the impact of the floaters on quality of life.
“Surgery for floaters is not undertaken lightly — it carries small but real risks including cataract acceleration and retinal detachment. It is reserved for patients with genuinely significant and persistent visual disability.”
Frequently Asked Questions
Your Journey from Symptoms to Solution
New or sudden floaters warrant same-day assessment to exclude a retinal tear. Chronic floaters can be assessed at a routine appointment.
Not all floaters need treatment. Mr Henderson gives you a clear, honest assessment of whether surgery is warranted — and what realistic improvement to expect.
Minimally invasive vitrectomy at Moorfields — the most effective treatment for significant floaters. Performed personally by Mr Henderson as a day case.
Most patients notice dramatic improvement immediately. Follow-up is structured and personal throughout your recovery.
“Floaters had been ruining my vision for two years — reading, driving, working on a screen. Mr Henderson was straightforward about the risks and benefits, and the surgery was transformative. I genuinely hadn’t realised how much they were affecting me until they were gone.”
Arrange a Consultation
Mr Henderson personally performs all vitrectomy surgery for floaters. There is no delegation to junior colleagues.
To arrange an assessment for floaters, please contact Alison Anscombe, Mr Henderson’s secretary:
+44 7974 015691 · alison.anscombe1@nhs.net
Or use the contact form on this website.