Why choose Mr Henderson for diabetic eye disease?
Mr Henderson manages the full spectrum of diabetic retinal disease — from laser and intravitreal injections through to complex vitrectomy for tractional retinal detachment and vitreous haemorrhage, including patients who have had previous surgery. He practises at Moorfields Eye Hospital, the UK’s leading centre for diabetic retinal disease. Book a consultation.
Diabetic Retinopathy
Diabetic retinopathy is the most common cause of preventable blindness in working-age adults in the UK. Early detection and timely treatment prevent the majority of cases of serious visual loss.
How Diabetes Affects the Eyes
High blood sugar levels damage the tiny blood vessels supplying the retina. Over time, these vessels leak fluid, bleed, or close off entirely — starving the retina of oxygen. In response, the retina attempts to grow new blood vessels, but these fragile new vessels are prone to bleeding and can cause devastating complications including vitreous haemorrhage and tractional retinal detachment.
Diabetic retinopathy can affect anyone with type 1 or type 2 diabetes. The longer the duration of diabetes and the poorer the blood sugar control, the greater the risk. Annual diabetic eye screening is essential to detect changes before symptoms develop.
“The tragedy of diabetic retinopathy is that by the time patients notice visual symptoms, significant damage may already have occurred. Screening saves sight.”
Stages of Diabetic Retinopathy
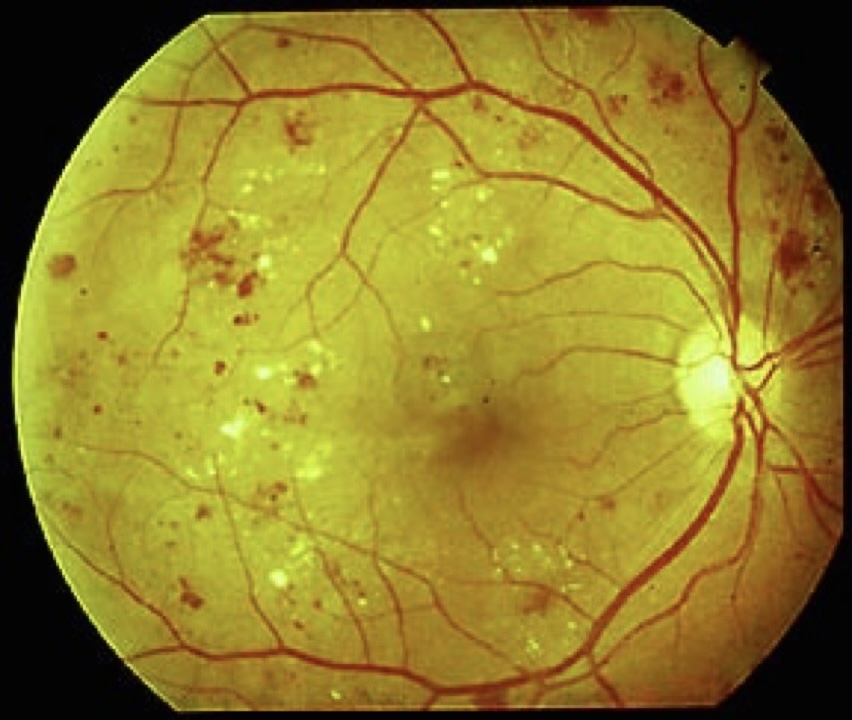
Background DR
Microaneurysms and small haemorrhages visible on examination. No impact on vision. Good blood sugar and blood pressure control is the key intervention.
Diabetic Maculopathy
Fluid leaks into the central macula (diabetic macular oedema), causing blurred central vision. Treated with intravitreal anti-VEGF injections.
Proliferative DR
New abnormal blood vessels grow on the retinal surface. High risk of vitreous haemorrhage and tractional retinal detachment. Treated with pan-retinal photocoagulation (PRP) laser.
When Surgery is Needed
Most diabetic retinopathy is managed with injections and laser. However, surgery becomes necessary when complications develop:
Vitreous haemorrhage — when new vessels bleed into the vitreous cavity, causing sudden severe visual loss. Vitrectomy removes the blood and allows treatment of the underlying vessels.
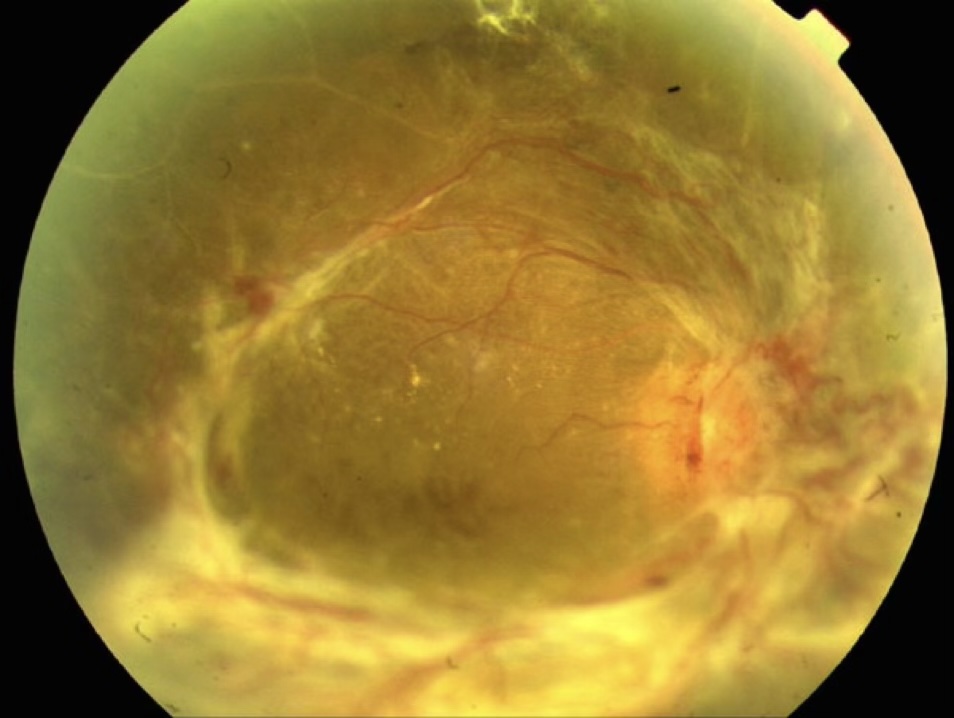
Tractional retinal detachment — fibrous tissue forming on the retinal surface contracts and pulls the retina away from the back of the eye. Complex vitrectomy with membrane peeling is required to relieve the traction and reattach the retina.
Diabetic vitrectomy is amongst the most technically demanding in retinal surgery. Mr Henderson has subspecialty expertise in complex diabetic cases.
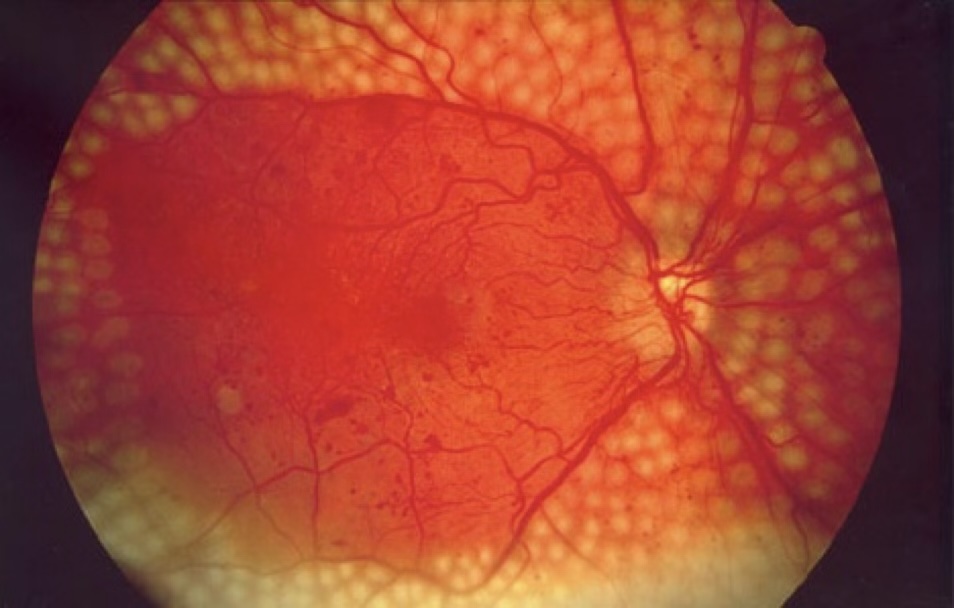
Pan-Retinal Photocoagulation
PRP laser treatment is used for proliferative diabetic retinopathy to reduce the drive for abnormal new vessel growth. Laser burns are applied to the peripheral retina, reducing its oxygen demand and causing regression of new vessels.
PRP is typically delivered over one to three sessions. It is not a cure, but effectively reduces the risk of vitreous haemorrhage and tractional detachment when performed at the right time.
Frequently Asked Questions
Your Journey from Assessment to Treatment
Comprehensive examination and OCT imaging to grade your retinopathy and identify any areas of concern — including macular oedema or new vessel growth.
Mr Henderson tailors a plan to your specific stage — monitoring, laser photocoagulation, anti-VEGF injections, or vitrectomy for advanced cases.
All treatment performed personally by Mr Henderson at Moorfields Eye Hospital — the UK’s leading centre for retinal disease.
Structured follow-up aligned with your diabetic care. Mr Henderson coordinates with your diabetes team to optimise your long-term outcomes.
“I’d been told my diabetic eye disease was getting worse and I might lose my vision. Mr Henderson started me on injections immediately and my sight has improved significantly. His ability to explain things clearly and without alarm made all the difference.”
Arrange a Consultation
Mr Henderson provides personal continuity of care for all diabetic eye disease patients. Your appointments are always with him directly.
To arrange an assessment for diabetic retinopathy, please contact Alison Anscombe, Mr Henderson’s secretary:
+44 7974 015691 · alison.anscombe1@nhs.net
Or use the contact form on this website.