Why choose Mr Henderson for retinal detachment?
Mr Henderson performs emergency and elective retinal detachment repair at Moorfields Eye Hospital — one of the world’s highest-volume retinal detachment centres. He offers the full surgical repertoire: vitrectomy, scleral buckling, and combined approaches, tailored to the specific characteristics of your detachment. Patients are seen urgently and surgery is arranged within 48 hours where required. As a consultant vitreoretinal surgeon in London, he performs all surgery personally.
Retinal Detachment — Emergency Surgery in London
Retinal detachment is a sight-threatening emergency. When the retina separates from the back of the eye, vision is lost rapidly and permanently unless treated urgently. With prompt surgery, the majority of patients regain useful vision.
Understanding Retinal Detachment
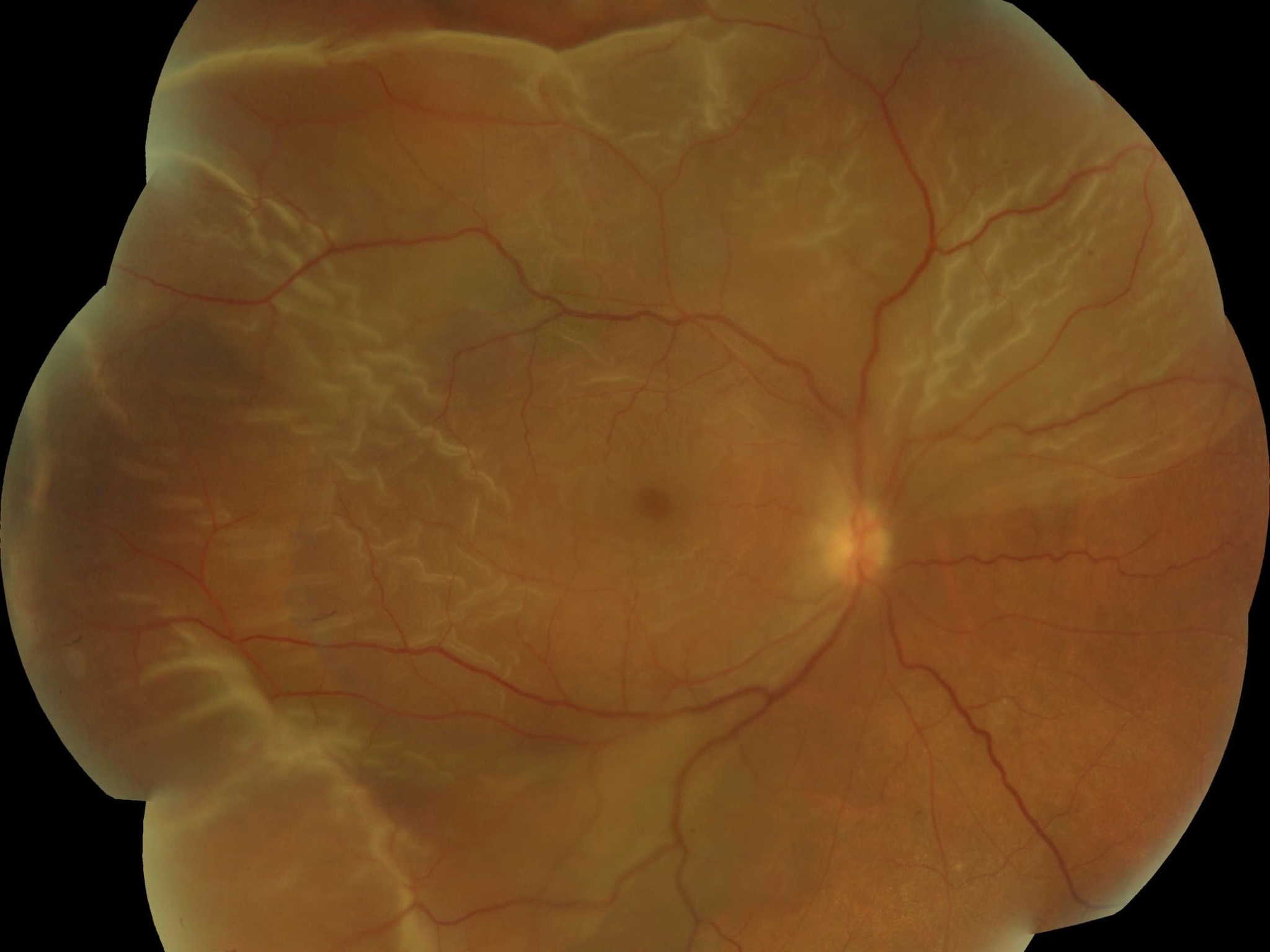
The retina is a thin layer of light-sensitive tissue lining the inside of the eye. Like wallpaper peeling from a wall, a detached retina separates from its underlying support layer — the retinal pigment epithelium — cutting off its blood supply and causing rapid, irreversible cell death.
The most common type is a rhegmatogenous retinal detachment, caused by a tear or hole in the retina that allows fluid from the vitreous cavity to seep underneath and lift the retina away. Risk factors include short-sightedness (myopia), previous eye surgery, eye trauma, and a family history of retinal detachment.

Symptoms to Watch For
Symptoms can develop suddenly and progress rapidly. Knowing the warning signs can be sight-saving.
Surgical Repair
All retinal detachments require surgery. The goal is to close the tear or tears responsible for the detachment, drain the fluid underneath, and reattach the retina to the back of the eye. Mr Henderson selects the most appropriate technique based on the pattern of detachment, the location of the tear, and the individual patient.
“The most important factor in achieving a good visual outcome is speed — the sooner a detachment is repaired before the macula detaches, the better the prognosis for central vision.”
Where the macula has already detached, surgery is still worthwhile and frequently results in meaningful visual recovery, though the final outcome takes longer to determine.
Surgical Techniques
Your Journey from Diagnosis to Recovery
Same-day or next-day consultation at Moorfields. Imaging, examination, and a clear diagnosis with no waiting.
Mr Henderson personally reviews your case and selects the technique best suited to your detachment — vitrectomy, scleral buckle, or pneumatic retinopexy.
All surgery is performed personally by Mr Henderson in the specialist theatres at Moorfields Eye Hospital — the world’s foremost eye hospital.
Most patients go home the same day. Mr Henderson follows your recovery personally, with structured appointments to monitor healing and vision.
Vitrectomy
The most versatile approach. The vitreous gel is removed, the retina reattached, and a gas or silicone oil tamponade used to hold it in place while it heals. Suitable for the majority of detachments.
Scleral Buckle
A silicone band is sutured around the outside of the eye to indent the wall, closing the tear from the outside. Particularly effective for younger patients and specific tear patterns.
Pneumatic Retinopexy
A gas bubble is injected into the eye and the patient positions to push the bubble against the tear. Suitable for selected cases with a single superior tear and minimal fluid.
Frequently Asked Questions
“I woke up on a Sunday with a curtain across my vision. Mr Henderson operated the following morning at Moorfields. Six weeks later my vision had recovered to the point where I could drive again. I cannot overstate how grateful I am for the speed and skill of his care.”
Arrange an Urgent Assessment
Mr Henderson personally performs all retinal detachment surgery. There is no delegation to junior colleagues.
If you are experiencing symptoms of retinal detachment, please seek urgent assessment. To contact Mr Henderson’s team:
+44 7974 015691 · alison.anscombe1@nhs.net
Or use the contact form on this website.