Epiretinal Membrane Surgery in London
An epiretinal membrane is a thin layer of scar tissue that forms on the surface of the macula, causing distortion and blurring of central vision. Surgery to remove it is highly effective and most patients experience meaningful visual improvement.
What is an Epiretinal Membrane?
An epiretinal membrane (ERM) — also called a macular pucker or cellophane maculopathy — forms when cells migrate onto the surface of the macula and lay down a thin sheet of contractile scar tissue. As this membrane contracts, it distorts the underlying retinal architecture, causing the characteristic wrinkling and visual symptoms.
Most ERMs arise from an anomalous posterior vitreous detachment, where residual vitreous cells remain on the retinal surface rather than detaching cleanly. Less commonly, they occur secondary to other eye conditions such as retinal tears, inflammation, or vascular disease.
ERMs are common, affecting around 2% of the population and becoming more prevalent with age. Many cause only mild symptoms and can be monitored. Surgery is recommended when visual disturbance becomes significant enough to affect daily activities.
Symptoms of Epiretinal Membrane (Macular Pucker)
The most common symptom is distorted vision — straight lines appear wavy, bent or curved. This is known as metamorphopsia — straight lines appear wavy or bent. This is particularly noticeable when looking at tiled floors, door frames, or printed text. Other symptoms include blurred or reduced central vision, images appearing slightly larger in one eye than the other (monocular diplopia), and difficulty with fine detail tasks such as reading.
“Distortion typically improves before the blur does after surgery. Patients often notice the metamorphopsia settling within the first few weeks, while the sharpness of vision continues to improve over months.”
Symptoms often progress slowly over months to years. Some patients experience an initial period of worsening after surgery as the retina recovers — like a crumpled piece of paper slowly flattening out — before meaningful improvement begins, typically within two to six weeks.
Vitrectomy and Membrane Peel
Surgery involves a minimally invasive vitrectomy using fine 25-gauge instruments. The vitreous gel is removed to provide access to the retinal surface, and the epiretinal membrane is carefully peeled away using fine forceps under the operating microscope. The internal limiting membrane (ILM) is also typically peeled to prevent recurrence.
The procedure is performed as a day case under local anaesthetic and takes approximately 30–45 minutes. There is no gas or posturing required after ERM surgery, which makes the recovery more straightforward than macular hole surgery.
Visual improvement continues for up to 12 months after surgery. The degree of improvement depends on how long the membrane has been present and the extent of underlying retinal distortion, but the majority of patients experience worthwhile gains in both acuity and distortion.
Frequently Asked Questions
Your Journey from Diagnosis to Recovery
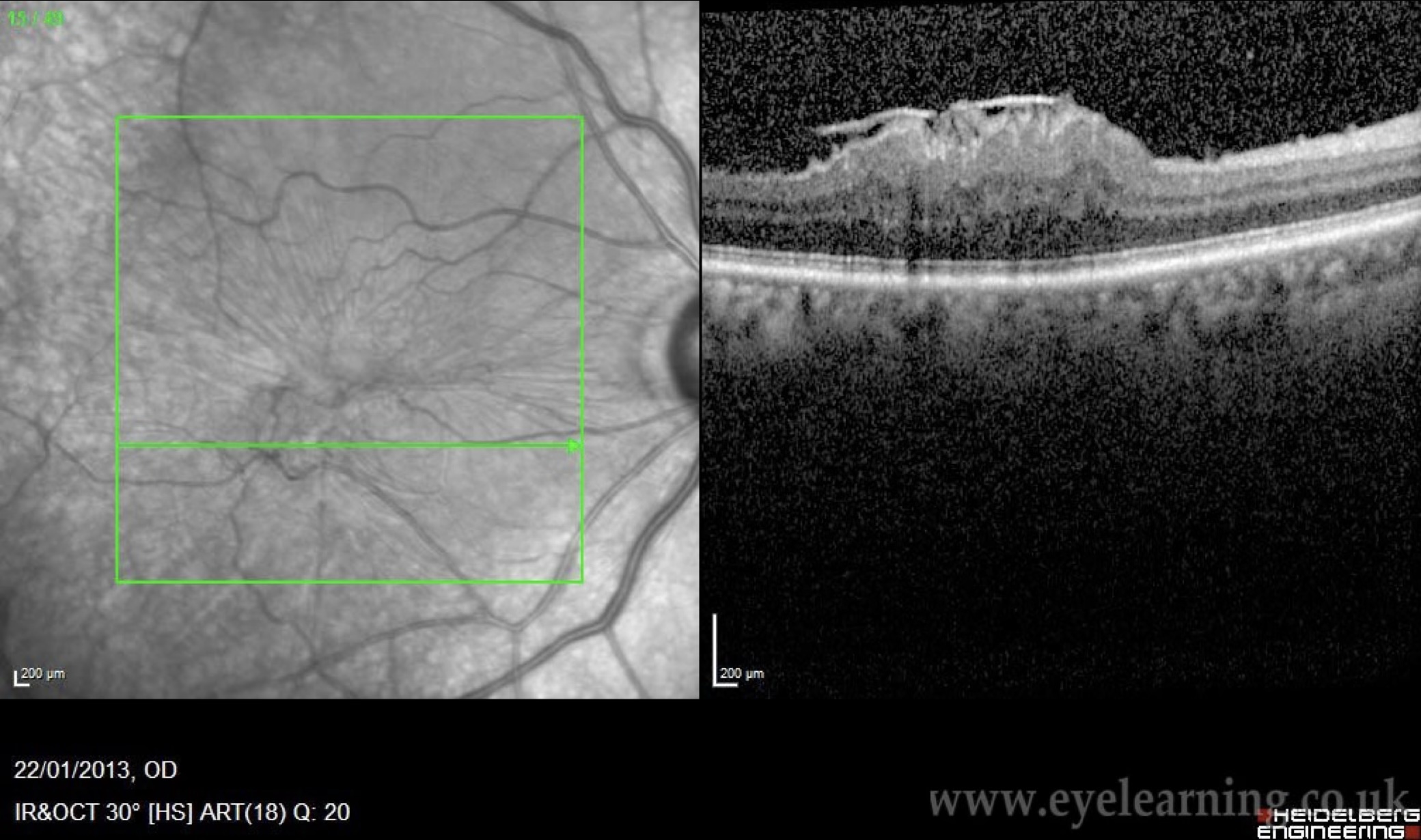
OCT scanning maps the membrane precisely. Many ERMs can be monitored — Mr Henderson will advise honestly whether surgery is needed now or can wait.
Surgery is recommended only when symptoms meaningfully affect daily life. Mr Henderson discusses the realistic timeline for improvement so you can plan.
25-gauge vitrectomy and membrane peel at Moorfields, under local anaesthetic. No gas, no posturing. Home the same day.
Distortion typically begins to settle within weeks; visual acuity improves over up to 12 months. Mr Henderson follows your recovery personally throughout.
“I’d been struggling with wavy, distorted vision for over a year and was told it would only get worse. Mr Henderson explained everything clearly — the surgery, the recovery, what to expect. Three months on, the distortion has largely gone. I wish I hadn’t waited so long.”
Arrange a Consultation
Mr Henderson personally performs all epiretinal membrane surgery. There is no delegation to junior colleagues.
To arrange an assessment for epiretinal membrane, please contact Alison Anscombe, Mr Henderson’s secretary:
+44 7974 015691 · alison.anscombe1@nhs.net
Or use the contact form on this website.